

Filling the tear trough with hyaluronic acid: anatomy, qualification and complications
Introduction
Filling the tear trough with hyaluronic acid used to be a routine procedure, but today it is approached much more cautiously. How should we think about it now? Should we actually abandon this treatment — or rather learn how to qualify and perform it safely? In this article, we discuss the key aspects: anatomy, technique, possible complications, and the criteria for qualifying or disqualifying patients.

Tear trough anatomy
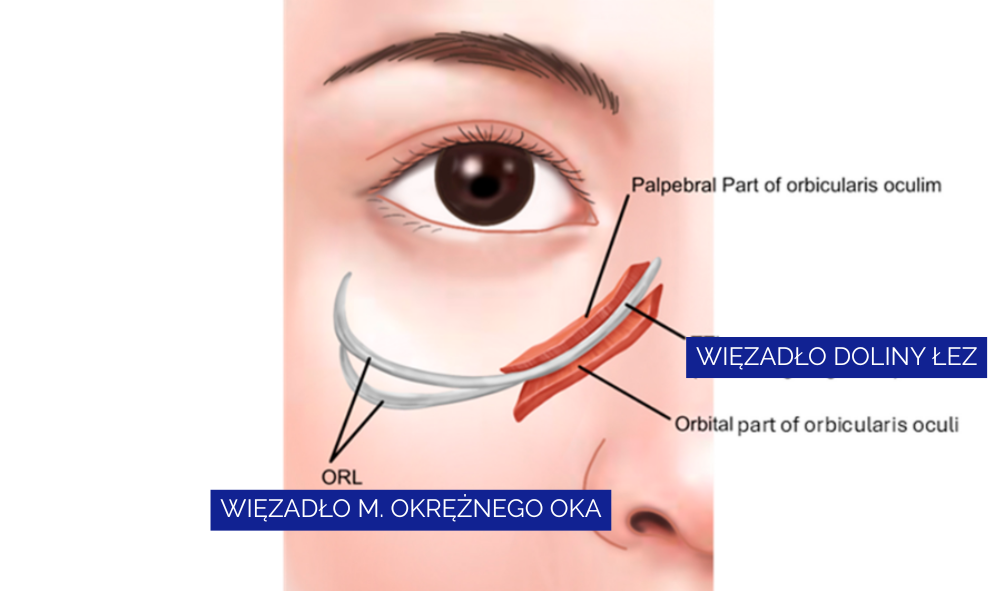
The tear trough is the depression running from the medial canthus toward the mid-cheek. It follows the course of the tear trough ligament, which is an extension of the orbicularis retaining ligament (ORL), usually located 2–3 mm below the orbital rim. This area contains only a trace amount of subcutaneous fat; the muscular layer is dominated by the orbicularis oculi muscle.
Lymphatic drainage and injection technique
In the lower eyelid, two lymphatic networks are described: the superficial system (both medially and laterally) and the deep system (so far described only laterally). This has practical significance because pressure from the filler implant on lymphatic vessels may cause chronic lower-eyelid edema. To reduce this risk, injecting in the supraperiosteal plane, beneath the orbicularis oculi muscle, is recommended — a layer in which lymphatic vessels are not present.
Injection layers and the risk of Tyndall effect
The lower eyelid skin is only about 0.3–0.5 mm thick, and subcutaneous fat is minimal in this region. Injecting filler subcutaneously, above the orbicularis oculi muscle, increases the risk of lumps, irregularities, and visibility of the product, which may result in the Tyndall effect.

PHAREE: recurrent eyelid edema after HA
One significant complication is chronic, recurrent lower-eyelid edema following hyaluronic acid injections (PHAREE — post-hyaluronic acid recurrent eyelid edema). Edema may occur shortly after the procedure or even many years later. It has a low chance of resolving spontaneously, so proper diagnostics (ideally ultrasound) and treatment with hyaluronidase are required.
In the past, this condition was often unrecognized, leading to long-lasting problems and extensive searches for the cause — frequently old, retained filler. Today we know that PHAREE is possible and relatively common, which is why discussing the risk and obtaining informed consent are essential parts of the consultation.

Patient qualification and disqualification
Careful qualification is crucial for safety and optimal outcomes. Pay attention to:
- Quality of the periorbital skin — loose, thin, or lax skin (more common in older patients) increases the risk of irregularities and edema.
- Hydration level of the lower eyelid skin — use the simple snap-back test: gently pull the lower eyelid skin and release; 1–2 seconds is considered normal. A longer return time suggests dehydration and excessive laxity; consider revitalizing treatments before filler.
- Appearance of the midface — the tired look may result from deflation of cheek fat compartments rather than the tear trough itself.
- Other periorbital concerns — a prominent lower-eyelid fat herniation may mimic a deep tear trough; in such cases, surgical consultation is recommended, as injections rarely provide a satisfactory long-term result.
- Tendency toward eyelid edema — in patients with pre-existing swelling, HA injections will almost certainly worsen the problem.

Practical tips to reduce risk
- Prefer the supraperiosteal plane, under the orbicularis oculi muscle, to reduce pressure on lymphatic vessels.
- Avoid subcutaneous injections above the orbicularis oculi muscle to minimize lumps, irregularities, and the Tyndall effect.
- Discuss the risk of PHAREE with the patient; in case of edema, consider ultrasound assessment and hyaluronidase treatment.
Summary
Tear trough filling is technically demanding, carries a risk of complications — including delayed ones — and requires great caution in patient qualification. Should it be performed? The decision belongs to the physician. The procedure is still widely used worldwide, is considered relatively safe, and — with proper qualification — can produce fast, long-lasting, and often spectacular results that cannot always be achieved with other minimally invasive methods.